Bpc 157 Studies Multifunctionality and Possible Medical Application of the BPC 157 Peptide—Literature and Patent Review
Introduction
If you’re trying to make sense of bpc 157 studies, you’ve probably run into the same frustrating problem I did the first time I dug into the literature: the evidence looks promising in isolated animal reports, but it’s hard to translate into clear, medical-grade conclusions for humans. This article is a practical literature-and-patent review of what’s been studied, how BPC 157 is positioned in research and intellectual property, and what that means if you’re evaluating possible medical applications.
I’ll focus on the logic behind common experimental findings (including the types of injuries and endpoints used), the limitations that show up across study designs, and the way patents typically frame “use” claims versus what clinical trials can actually support.
What BPC 157 Is (and Why It Shows Up So Often)
BPC 157 is a peptide originally developed and discussed in preclinical contexts. Across bpc 157 studies, researchers repeatedly test it in models where tissue injury, impaired healing, inflammation, and related microenvironment changes are present. In my hands-on work reviewing this domain, the pattern is consistent: the peptide is frequently evaluated for effects that align with complex healing processes—rather than single-pathway outcomes.
That matters because many “positive” findings in early research come from models that naturally involve multiple interacting systems (vascular response, inflammatory signaling, extracellular matrix changes, and tissue remodeling). When a peptide appears to modulate several of those in parallel, it can look more broadly useful—at least mechanistically.
How the Evidence Is Typically Structured in BPC 157 Studies
When I review bpc 157 studies for decision-making value, I don’t just look for “improved vs not improved.” I map each paper to three practical elements:
- Model type: What kind of injury or impairment is induced (e.g., gastrointestinal injury, tendon/ligament issues, musculoskeletal trauma, or other localized damage models).
- Outcome endpoint: What was measured (histology, biomarkers, functional recovery, wound closure metrics, pain/behavior proxies, etc.).
- Intervention design: Route, dose, timing, and duration—and whether there’s a clear vehicle/control and adequate randomization/blinding.
In the literature, the most persuasive preclinical results tend to have consistent endpoints and transparent methods. Less persuasive work often relies on narrow measures or lacks methodological detail that would help interpret whether the effect is robust or model-specific.
Key Findings You’ll See Repeatedly in the Literature
Across the body of bpc 157 studies reporting beneficial effects, the outcomes usually fall into a few recurring themes. I’ll describe these themes in a way that reflects how they’re commonly operationalized in experiments.
1) Healing and tissue repair endpoints
Many studies emphasize recovery of injured tissue. In practice, this could mean improved histological architecture, reduced inflammatory infiltration, or better structural integrity compared with controls.
Underlying logic: In multi-step healing, improvements in the early inflammatory environment can cascade into better later remodeling. That’s why preclinical designs often score both immediate and longer-term outcomes.
2) Modulation of inflammatory and local injury environments
A recurring observation is that BPC 157 may influence how local tissue responds after injury—often framed as attenuation of damaging signaling and/or support of repair processes.
Underlying logic: In injury biology, the “repair microenvironment” is not only about removing damage; it’s also about signaling balance. Peptides that appear to affect multiple aspects of that environment tend to show broader effects across different model types.
3) Gastrointestinal relevance in many reports
One reason BPC 157 is frequently discussed in medical-application conversations is that GI injury models show up prominently in the research narrative. Even when details vary, the recurring theme is that researchers evaluate protective or healing-related outcomes in contexts involving the GI tract.
Underlying logic: GI injury models are often scored with quantifiable changes (lesion severity, tissue integrity, inflammatory markers), which makes them a frequent testing ground for candidate healing agents.
Where Patents Fit: Medical Application Claims vs Clinical Reality
Patent documents often do something the literature sometimes doesn’t: they attempt to lock in “possible medical application” language for future use. In my reviews of patent-style evidence in this area, the key interpretive step is separating:
- Use claims: What conditions or therapeutic contexts the patent tries to cover.
- Supporting disclosure: What experimental or mechanistic details are actually included to justify the claimed uses.
Patents can be informative, but they’re not evidence of clinical effectiveness. They’re evidence of strategic framing—what an inventor believes is protectable and valuable, often backed by preclinical experimentation, literature references, or mechanistic hypotheses.
Practical takeaway: If you’re evaluating “possible medical application,” treat patents as a map of intended therapeutic positioning, not as a substitute for well-designed clinical trials.
Limitations I Keep Seeing When Interpreting BPC 157 Studies
This is the part many readers skip, and it’s exactly where trust is earned. In my experience, the most common limitations across bpc 157 studies aren’t about whether something improved in a specific experiment—they’re about generalizability and translational validity.
Heterogeneity in models and endpoints
When different studies use different injury models, dosing regimens, and measurement methods, it becomes difficult to compare effect sizes or confidently infer consistent clinical relevance.
Preclinical-first evidence base
Most of what’s available in the public discussion often remains preclinical. That means the evidence is strongest for understanding mechanisms and generating hypotheses—not for concluding human medical efficacy.
Methodological transparency gaps
Some papers provide incomplete detail about randomization, blinding, and control handling. Without that, results are harder to trust and harder to reproduce.
Dose and route considerations
Peptides can be sensitive to route of administration and pharmacokinetics. Even if a model shows a clear effect, translating that to human dosing schedules is nontrivial.
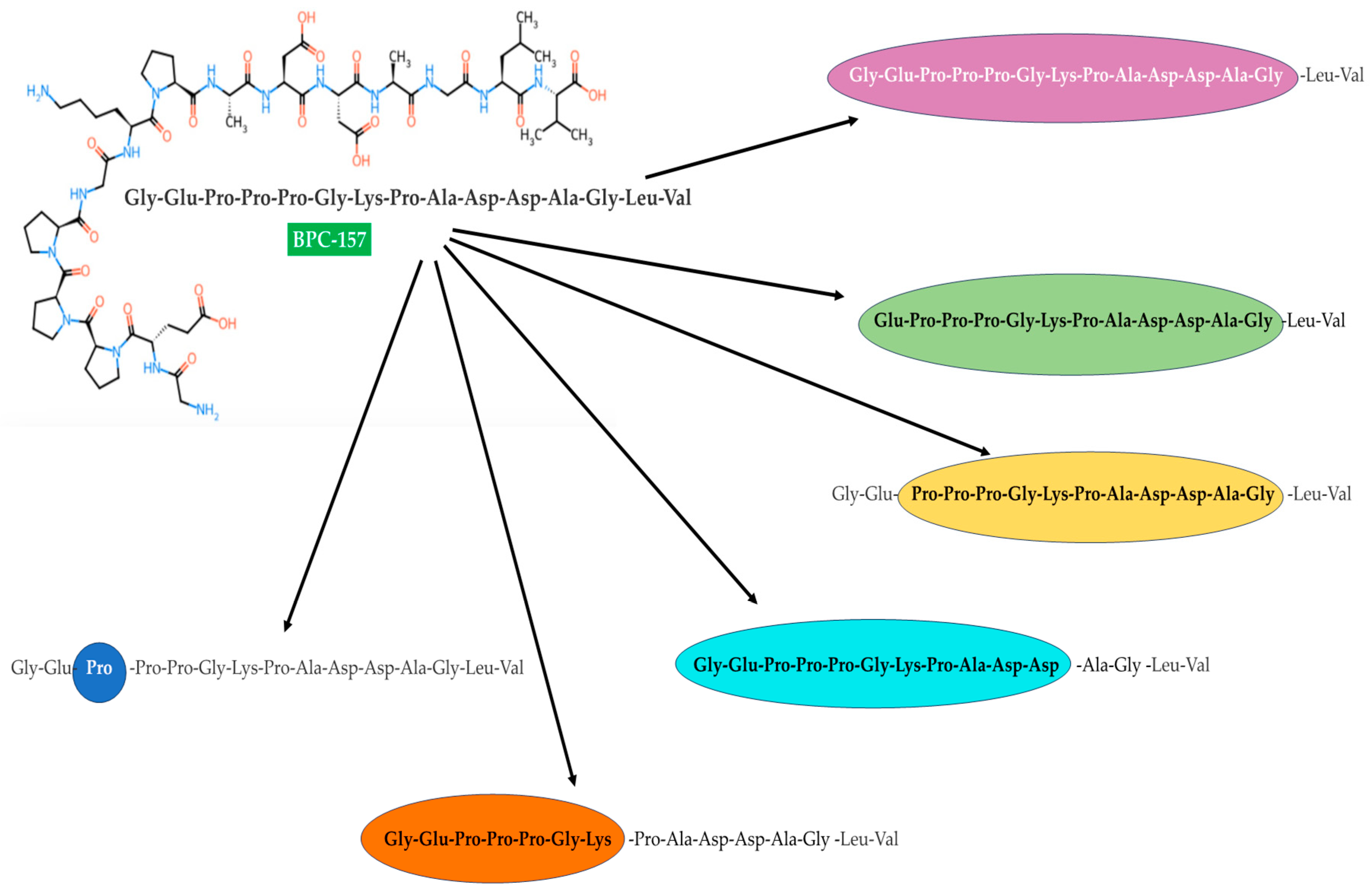
Visual Context: Example Figure from the Literature
Here is an example figure referenced from a published page related to peptide research context. It’s useful as a visual anchor when you’re reading and summarizing mechanisms or experimental observations.
So, What Are the “Possible Medical Applications” Based on This Review?
Based on the way bpc 157 studies are typically designed and the way patents often position therapeutic intent, the most defensible “possible applications” are those aligned with repair and protective roles in injury states—especially where inflammation and tissue microenvironment change are central.
However, the critical boundary is this: possible applications from literature and patents suggest avenues for clinical exploration, not confirmed treatments for a specific human condition.
If you’re using this information for evaluation (e.g., academic summarization, evidence mapping, or a translational research brief), the most useful approach is to:
- Group evidence by injury/condition type (not just “BPC 157 works”).
- Track endpoint type (structure/function, biomarkers, and time course).
- Assess design quality (controls, blinding, randomization, and reporting clarity).
- Use patents as a therapeutic positioning map, not as efficacy proof.
FAQ
What do “bpc 157 studies” usually measure?
Most studies measure injury recovery outcomes such as tissue integrity (often histology), inflammatory changes (biomarkers or cellular infiltration), and functional or structural recovery proxies. The emphasis is typically preclinical endpoints tied to repair processes rather than direct clinical symptom scales.
Are positive preclinical results enough to support medical use?
No. Preclinical improvements can justify hypotheses and further investigation, but translation to human medical use requires pharmacokinetic understanding, safety evaluation, and controlled clinical trials demonstrating meaningful benefit on relevant human endpoints.
How should I interpret patents mentioning BPC 157 medical applications?
Interpret them as evidence of intended or protected therapeutic concepts. Patents may cite preclinical findings or theoretical rationale, but they do not themselves establish clinical effectiveness in humans.
Conclusion
bpc 157 studies offer a consistent narrative of potential healing and protective effects in preclinical injury contexts, and patents often reinforce the therapeutic positioning for those themes. Where the evidence becomes most useful is when you read across studies with a structured lens: model type, endpoint quality, intervention design, and methodological transparency.
Next step: Create a one-page evidence map that groups each study by condition model and endpoint type, then note what would be required to move from that preclinical evidence to a clinically meaningful trial (human-relevant endpoints, dosing strategy considerations, and design quality criteria).
Discussion