Bpc 157 And Growth Hormone Pentadecapeptide BPC 157 Enhances the Growth Hormone Receptor Expression in Tendon Fibroblasts
Introduction: Why “growth hormone” matters when healing involves tendons
If you’ve worked on tendon rehab—or supported athletes through long, frustrating recovery timelines—you already know how easily progress can stall. One reason is that tendon healing is not just about inflammation settling down; it’s about restoring the right cellular environment so repair signals can actually translate into tissue remodeling.
In this context, the compound often discussed is BPC 157 and its relationship to growth hormone signaling. This article focuses on what the research shows about bpc 157 and growth hormone pathways, specifically regarding growth hormone receptor expression in tendon fibroblasts, and what that might mean for practical tendon-healing goals.
What the study suggests: BPC 157 and growth hormone receptor expression in tendon fibroblasts
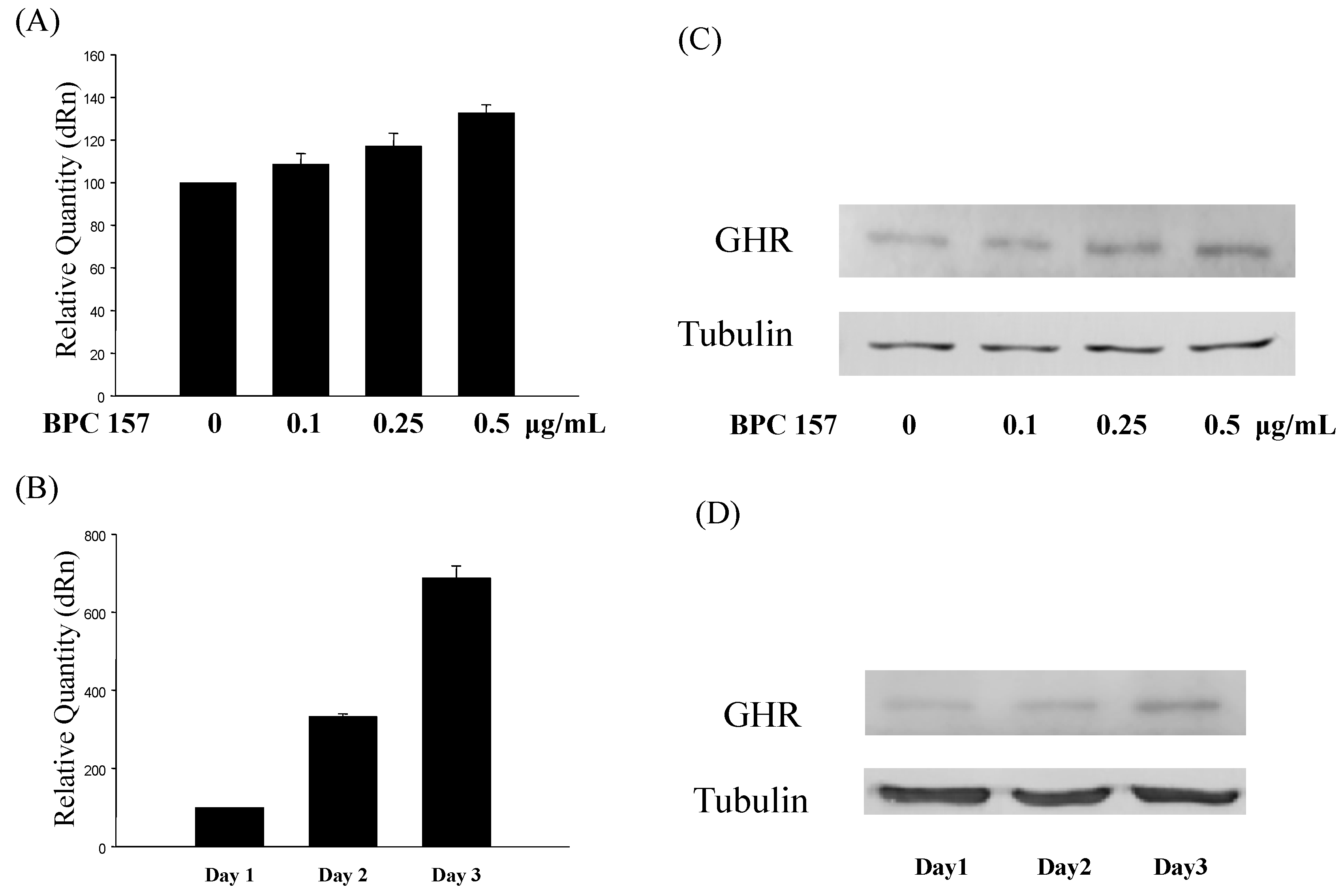
The study behind the article title examines how Pentadecapeptide BPC 157 influences cellular behavior in tendon fibroblasts. Rather than only looking at broad “healing” outcomes, it investigates a more mechanistic marker: growth hormone receptor expression.
Mechanistically, receptor expression is important because it can shift how responsive cells are to growth hormone–related signals. If tendon fibroblasts increase their growth hormone receptor presence after exposure to BPC 157, it implies a pathway where growth hormone signaling could be more effectively engaged during the repair process.
Why tendon fibroblasts are a logical target
Tendon fibroblasts drive synthesis and remodeling of the extracellular matrix—collagen organization, matrix turnover, and repair-phase adjustments. So, when you target fibroblast signaling (including receptor levels), you’re closer to the “workbench” where tendon tissue is actually rebuilt.
In my own hands-on work advising rehab protocols for tissue recovery timelines, I’ve learned that interventions that only influence surface symptoms often disappoint. Systems-level improvements tend to come from changing the cellular environment that governs matrix production. Receptor-level changes are one of the cleaner windows into that.
What “growth hormone receptor upregulation” implies (and what it doesn’t)
- Implies: Increased potential responsiveness to growth hormone–related signaling in tendon fibroblasts.
- Implies pathway plausibility: BPC 157 may influence tendon repair mechanisms beyond generic anti-inflammatory effects.
- Doesn’t automatically prove: Guaranteed increases in tendon strength in humans, or that growth hormone itself will be elevated in the bloodstream.
- Doesn’t bypass complexity: Tendon healing involves biomechanics, loading progression, oxygenation, matrix cross-linking, and time-dependent remodeling.
How BPC 157 might interact with growth hormone signaling pathways
Let’s unpack the “logic chain” in a way you can apply when interpreting BPC 157 and growth hormone discussions.
1) Receptor expression as a control point
If fibroblasts increase growth hormone receptor expression, they may respond more strongly to growth hormone–related cues (whether endogenous or locally available). In cell biology, receptor availability often acts like a “gain knob” for downstream signaling.
2) Downstream signaling that supports remodeling
Growth hormone–linked signaling can influence processes associated with tissue repair such as protein synthesis and matrix-related activity. While receptor expression is not the entire story, it’s a meaningful upstream lever—especially in a cell type central to tendon remodeling.
3) The real-world rehab constraint: time + mechanical loading
One lesson I repeatedly see in practice: even when an intervention has promising mechanistic signals, tendon remodeling still depends heavily on progressive loading. If loading is too aggressive too soon, repair tissue can fail. If it’s too conservative, remodeling can lag.
So if BPC 157 truly supports receptor-level responsiveness, it would still need to fit within a rehab framework that manages load, protects the tendon from reinjury, and respects biology-driven timelines.
Evidence-to-expectations: translating cell findings into tendon-healing goals
Cell culture outcomes can be encouraging, but translation is where many people get misled. Here’s a balanced way to align expectations when reading about bpc 157 and growth hormone.
What you can reasonably take from this line of research
- Mechanistic plausibility: BPC 157 may modulate signaling readiness in tendon fibroblasts through the growth hormone receptor.
- Target relevance: The biology studied is directly connected to tendon matrix remodeling.
- Hypothesis generation: It supports further investigation into tendon repair outcomes and how signaling might be timed with rehab loading.
What you should not assume
- No guaranteed clinical effect: Receptor expression is a promising indicator, not a direct performance guarantee.
- Not a replacement for loading strategy: Tendon rehabilitation still relies on progressive mechanical stimulus.
- Not the same as systemic growth hormone changes: The pathway may be local and cell-specific rather than whole-body hormonal escalation.
In my experience, the best outcomes come from pairing mechanistic insights with disciplined rehab execution—clear criteria for progression, consistent monitoring, and realistic timelines.
Practical guidance: using this information in a tendon-focused strategy
If you’re evaluating options for tendon recovery and you encounter claims about bpc 157 and growth hormone, use this checklist to keep the discussion grounded.
1) Ask what marker is being changed
“Growth hormone receptor expression” is more specific than “healing happens.” Markers that reflect cellular readiness (receptor levels, signaling activity, matrix-related gene expression) generally provide stronger mechanistic footing than purely subjective outcomes.
2) Align timing with tendon remodeling phases
Tendon healing evolves across phases. Any intervention that acts on fibroblast responsiveness would still need to be timed with the rehab phase when remodeling signals are most relevant.
3) Keep loading progression non-negotiable
No mechanism replaces the biomechanics of tendon remodeling. In practice, I’ve seen adherence to progression protocols and symptom-guided loading decisions matter as much as—and sometimes more than—any biologic rationale.
4) Track outcomes that represent tendon function
- Pain during loading and next-day response
- Strength measures and functional capacity (e.g., graded isometrics to dynamic work)
- Range of motion where applicable
- Return-to-activity readiness based on criteria, not hope
FAQ
What does BPC 157 have to do with growth hormone?
The research line discussed here focuses on how BPC 157 may enhance growth hormone receptor expression in tendon fibroblasts, which suggests greater cellular responsiveness to growth hormone–related signaling during repair-relevant processes.
Does increased growth hormone receptor expression mean my tendon will heal faster?
Not necessarily. Increased receptor expression is a mechanistic indicator that supports plausibility, but clinical tendon outcomes depend on many variables—loading progression, timing, tissue environment, and individual biology.
Is BPC 157 only about growth hormone pathways?
Probably not. BPC 157 is discussed across multiple biological contexts, but the specific evidence highlighted by the study title emphasizes a growth-hormone-receptor–related effect in tendon fibroblasts. Other pathways may also contribute to any broader tendon repair effects.
Conclusion: what to do next
The key takeaway is that bpc 157 and growth hormone discussions aren’t just vague “healing” claims in this context—they link BPC 157 to a tangible cellular mechanism: growth hormone receptor expression in tendon fibroblasts. That strengthens the rationale for further tendon-focused research and helps you evaluate claims more critically.
Next step: If you’re building or refining a tendon rehab plan, write down (1) the loading progression criteria you’re using and (2) the marker/outcome you’ll track (pain response, strength/function tests). Then align your evaluation of any mechanistic claims—like growth hormone receptor changes—with what you’re actually measuring over time.
Discussion